
Originally published in: Journal of Substance Abuse Treatment
April, 2015 – Volume 51, Pages 53–58
Authors: Peter J. Kelly, Ph.D, Frank P. Deane, Ph.D, Amanda L. Baker, Ph.D
Received: April 14, 2014; Received in revised form: October 20, 2014
Accepted: October 27, 2014
Published Online: November 04, 2014
Article Outline
1. Introduction
2. Materials and methods
2.1. Participants
2.2. Measures
2.2.1. Background information
2.2.2. Problematic behaviours
2.2.3. Mental health
2.2.4. Cognitive behavioral skills
2.2.5. Group cohesion
2.2.6. Quality of facilitation
2.2.7. Homework
2.3. Procedures
2.4. Statistical analysis
3. Results
3.1. SMART Recovery participants
3.2. Problematic behaviours
3.3. Mental health
3.4. Use of cognitive behavioral skills, group cohesion, quality of group facilitation and homework
3.5. Predicting the use of cognitive behavioral skills
4. Discussion
Highlights
- SMART Recovery groups are cognitive–behaviourally oriented mutual support groups for individuals with addictions.
- Participants attending SMART Recovery present with a complex clinical profile, including high rates of self reported co-occurring mental illness.
- Participants were more likely to report the use of cognitive restructuring than behavioural activation.
- Group cohesion was positively correlated with the use of both cognitive and behavioural skill utilisation by participants attending SMART Recovery.
Abstract
SMART Recovery groups are cognitive–behaviourally oriented mutual support groups for individuals with addictions. The aim of the study was to assess the extent to which the quality of group facilitation, group cohesion and the use of between session homework activities contribute to self-rated use of cognitive–behavioural skills amongst group participants. Participants attending SMART Recovery groups in Australia completed a cross-sectional survey (N = 124). The survey included measures of cognitive and behavioural skill utilisation, group cohesion, quality of group facilitation and a rating of how frequently participants leave group meetings with an achievable between session homework plan. On average, participants had been attending SMART Recovery meetings for 9 months. Participants were most likely to attend SMART Recovery for problematic alcohol use. Regression analyses indicated that group cohesion significantly predicted use of cognitive restructuring, but that only provision of homework at the end of each group session predicted self-reported behavioural activation. Both group cohesion and leaving a group with an achievable homework plan predicted participant use of cognitive behavioural skills. The concrete actions associated with homework activities may facilitate behavioural activation. There is a need for longitudinal research to examine the relationship between the utilisation of cognitive and behavioural skills and participant outcomes (e.g. substance use, mental health) for people attending SMART Recovery groups.
1. Introduction
Mutual support groups are the most widely accessed form of alcohol or other substance abuse treatment (Dawson et al., 2006, Kessler et al., 1997). The major advantages of mutual support groups are that they are cost-effective to deliver, they are generally easy to access and free of charge for participants, and they are able to provide ongoing continuing care (Kelly, Magill, & Stout, 2009). The large majority of mutual support groups use the 12-step approach (e.g. Alcoholics Anonymous, Narcotics Anonymous). Consequently, research examining mutual support groups has largely focused on 12-step meetings, where they have been demonstrated to be at least as effective as other types of therapeutic interventions (see Kelly et al., 2009 for review). Twelve step groups also appear to improve treatment outcomes for people who are accessing other types of formal treatment (Dawson et al., 2006) or following inpatient treatment for alcohol or substance use disorders (Gossop et al., 2003). Whilst there is increasing empirical support for the use of 12-step approaches, the importance of offering alternate types of mutual help groups has been highlighted in the literature (Horvath, 2000, Horvath and Yeterian, 2012). It is likely that there are a sub-section of participants who may not be willing to attend 12-step meetings for a range of philosophical reasons. For example, longitudinal research has identified that there are a range of client variables that predict early dropout from 12-step meetings. These client variables include having lower motivation for behaviour change, a low belief in the disease model of addiction, low religious affiliation, and limited previous involvement in 12-step groups (Kelly & Moos, 2003). It is probable, at least for a proportion of participants, that alternate approaches to 12-step groups may be beneficial.
Self-Management and Recovery Training (SMART Recovery) is a not-for-profit organisation that provides mutual help groups for people experiencing problematic behaviours (Horvath, 2000, Horvath and Yeterian, 2012). Incorporated as an organisation in 1992, by 2012 there were 698 SMART Recovery meetings being held regularly throughout the world (Allwood & White, 2013). SMART Recovery was originally developed as an alternative to 12-step approaches, with the major distinction being that SMART Recovery incorporated cognitive behavioural therapy (CBT) to promote positive behavioural change (Horvath, 2000). This includes helping participants to (1) identify the relationship between thoughts, feelings and behaviours; (2) challenge unhelpful thoughts and beliefs; (3) utilise positive behavioural strategies; and (4) use between group homework activities (referred to as achievable 7-day action plans in SMART Recovery). Whilst previous research has not examined the effectiveness of CBT within a SMART Recovery context, the utility of CBT approaches across alcohol and illicit substance abuse treatment has been well established (Magill & Ray, 2009).
Another major distinction between SMART Recovery and 12-step groups is that a facilitator leads each SMART Recovery group. The facilitator may be a professional or non-professional person, who has completed training in the SMART Recovery approach. The purpose of the facilitator is to maintain the structure of the meetings and to help facilitate active involvement of participants (Horvath & Yeterian, 2012). Whilst the theoretical framework used by SMART Recovery was intentionally developed to reflect current evidence based approaches (Horvath, 2000, Horvath and Yeterian, 2012), there has been a lack of published research specifically examining SMART Recovery (Horvath & Yeterian, 2012). The limited research to date has largely focused on comparisons between 12-step approaches and SMART Recovery. This research has included examining between group differences on specific variables such as religiosity, spiritual beliefs and locus of control (Atkins et al., 2007, Li et al., 2000). Additionally, one study compared outcomes for people diagnosed with a co-occurring mental illness who were alternatively assigned to SMART Recovery groups or 12-step groups (Brooks & Penn, 2003). Length of time attending mutual support groups, including SMART Recovery and 12-step groups, has been demonstrated to be positively associated with decreased substance use (Atkins & Hawdon, 2007).
Whilst the comparison of SMART Recovery groups and 12-step approaches is of importance, there has been a lack of research examining the ‘active ingredients’ associated with SMART Recovery. The identification and evaluation of ‘active ingredients’ has increasingly played a greater role in addiction research (Kelly et al., 2009, Moos, 2008, Morgenstern and Longabaugh, 2000), particularly as the field moves to refining current approaches and disseminating “elements that are essential to effective practice” (Miller, Sorensen, Selzer, & Brigham, 2006, p. 34). The use of cognitive and behavioural skills is considered to be the primary mechanism through which SMART Recovery participants make positive behavioural changes (Horvath & Yeterian, 2012). However, previous research has not examined the extent to which these skills are ‘actually’ used by participants. Understanding the use of these skills by participants is an important first step in starting to establish a specific evidence base for SMART Recovery. Likewise, research has not previously examined the factors that might promote the use of cognitive or behavioural skills by group members. With it being unlikely that SMART Recovery group facilitators are ‘experts’ in CBT, it is very important that the ‘active ingredients’ associated with successfully facilitating SMART Recovery groups are clearly articulated. This may provide an opportunity to further refine facilitator training or modify the current SMART Recovery approach. It is likely that the longer participants have been attending SMART Recovery groups, the more likely that they are to use cognitive and behavioural skills. However, it is possible that group processes might play an important role in helping to promote the use of these skills. Whilst it has not previously been examined, SMART Recovery group facilitators presumably play a primary role in encouraging participants to develop and utilise cognitive and behavioural skills. Additionally, as has been identified in research examining 12-step approaches, support from group members and the cohesion of the group are likely to play an important role in promoting the use of these skills (Moos, 2008). The use of between-session homework activities (i.e. ‘achievable 7-day action plans’) is a process level variable that is likely to promote the use of cognitive and behavioural skills. Homework has an extensive history in the broader psychotherapy literature (Kazantzis et al., 2000, Kazantzis et al., 2010) and is primarily used to help generalise skills developed in session to the person’s broader world.
The current study was conducted as a cross-sectional survey of people attending SMART Recovery groups across Australia. As this was the first study to examine SMART Recovery within an Australian context, the first aim was to provide a description of participants accessing these meetings. This will provide, for the first time, a description of the potential clinical complexities associated with people attending these groups and is likely to help inform an understanding of the needs of people accessing these groups. The second aim was to examine how frequently participants used cognitive and behavioural skills outside of group meetings. The third aim was to examine the variables that may predict participants’ self-reported use of cognitive and behavioural skills, as measured by the Cognitive–Behavioural Therapy Skills Questionnaire (Jacob, Christopher, & Neuhaus, 2011). It was hypothesised that the longer participants had attended the SMART Recovery meetings, the more likely they would be to use cognitive and behavioural skills. Additionally it was hypothesised that group factors (i.e. group cohesion and participants’ perceptions of the quality of group facilitation) and process factors (i.e. how regularly participants left sessions with homework) would also predict the use of cognitive and behavioural skills.
2. Materials and methods
2.1. Participants
All participants were attending SMART Recovery groups being conducted in Australia. At the time the survey was distributed, there were 104 active SMART Recovery groups. Due to the nature of the way SMART Recovery groups are organised and delivered, there is no central register of the number of participants who attend these groups. With group facilitators reporting that an average of about five to six participants attend each group (unpublished data collected by the research team), we estimate that approximately 582 people attend SMART Recovery each week in Australia. During the study period, 124 SMART Recovery participants completed the survey (approximately 21%).
2.2. Measures
Participants were asked to complete a detailed survey that was composed of the following measures sections:
2.2.1. Background information
Demographic information was collected including age, gender, country of birth, language spoken at home, and indigenous status. Participants were asked to report how long they had been attending SMART Recovery groups (months), how frequently they attended the groups, and whether they were currently attending any other types of treatment (i.e. 12-step groups, residential rehabilitation, detoxification, methadone maintenance, individual counselling or mental health services).
2.2.2. Problematic behaviours
Participants were asked to identify the problem behaviour(s) that caused them concern. Options included tobacco, alcohol, drug, sex, pornography, gambling, Internet, shopping or food addictions. Participants were asked more specifically about possible alcohol or other substance abuse problems, and “how long” the person has had “problems with alcohol or other substances of abuse” (years). They were also asked to identify the substance “currently” causing the greatest concern, and to identify the types of substances that they had used in the past 12-months.
2.2.3. Mental health
Participants were asked if they had “previously received treatment for a mental health problem” (yes/no), if they were “currently prescribed medication for any mental health conditions” (yes/no), if they had “ever attempted suicide” (yes/no) and if they had “attempted suicide in the last 30-days” (yes/no). Psychological health was assessed by the Kessler-10 (K10; Kessler et al., 2003). The K10 is 10-items in length. Each item is rated on a 5-point scale (1 = ‘none of the time’, 5 = ‘all of the time’). The items were summed to provide a total summed score that indicates the level of psychological distress. Items predominantly measure symptoms associated with depression (e.g. “In the last four weeks, about how often did you feel hopeless?”) and anxiety (e.g. “In the last four weeks, about how often did you feel nervous?”). The K10 has been widely used in population-based research and has been demonstrated to have good psychometric qualities (Andrews and Slade, 2001, Kessler et al., 2003). In the current study, the K10 was found to have high internal consistency (α = 0.95).
2.2.4. Cognitive behavioural skills
The Cognitive–Behavioural Therapy Skills Questionnaire (Jacob et al., 2011) was used to examine how frequently participants use cognitive and behavioural skills. The questionnaire was the first self report measure to be developed to assess the use of cognitive and behavioural skills for people presenting with “complex clinical profiles” (Jacob et al., 2011, p. 595). The questionnaire consists of two subscales: (1) cognitive restructuring (e.g. “find evidence to support my thoughts before buying into them”) and (2) behavioural activation (e.g. “engage in activity instead of a harmful behaviour”). The cognitive restructuring subscale has 9-items and the behavioural activation subscale as 7-items. All items in the questionnaire are rated from 1 (“I don’t do this”) to 5 (“I always do this”), with the items summed for each of the subscales. In the current study, both subscales had high internal consistency (cognitive restructuring, α = 0.90; behavioural activation, α = 0.87).
2.2.5. Group cohesion
Group cohesion was measured using the Group Climate Questionnaire (GCQ, MacKenzie, 1983). The GCQ has been used extensively in therapeutic research, and is the most widely used measure of group process (Johnson et al., 2006). To minimise burden on participants, only the Engagement Scale was used in the current study. This approach has previously been used to examine the role of group cohesion in mental health settings (Deane, Mercer, Talyarkhan, Lambert, & Pickard, 2012). This subscale is 5-items in length (e.g. “The group members liked and cared about each other”), and each item is rated from 0 (‘not at all’) to 6 (‘extremely’). A total score is obtained by summing the five items, with higher scores representing higher levels of group cohesion. In the current study, the GCQ Engagement Scale was found to have high internal consistency (α = 0.92).
2.2.6. Quality of facilitation
The participants’ perceived quality of the SMART Recovery group facilitation was examined using a 5-item measure taken from the 2010 SMART Recovery Participant Survey (SMART Recovery, 2014). This survey has previously been used to conduct a national survey of SMART Recovery participants attending groups in the United States. Participants were asked to rate their “regular SMART Recovery group facilitator” across six factors, namely (1) knowledge about SMART program, (2) patience with participants, (3) skills in guiding discussions, (4) ability to keep the group on track, (5) dealing with disruptive comments, and (6) creativity presenting and using tools. Items were rated from 1 (‘poor’) to 5 (‘excellent’). In the current study, the Quality of Facilitation Scale was found to have high internal consistency (α = 0.94).
2.2.7. Homework
A single-item homework question was used to examine the frequency with which participants leave each session with homework. The item was: “When I attend SMART Recovery groups I always leave each session with an achievable plan that can be completed during the next 7-days”. The question was rated from 1 (‘definitely false’) to 7 (‘definitely true’).
2.3. Procedures
In June 2013, hard copies of the research instruments were sent to each of the SMART Recovery group facilitators responsible for each meeting. Facilitators were encouraged to distribute the surveys to the group participants within a 1-month period. Participants were provided with a copy of the participant information sheet, survey and a reply paid envelope. Facilitators were provided with a standard script to introduce the survey. This script included providing the participants with information on who was conducting the study, the voluntary and anonymous nature of the survey and instructions to return the survey. Participants were encouraged to either complete the survey at the end of their group meeting or to complete the survey at home. The surveys were returned to the research team at the University of Wollongong. Group members were informed that participation was entirely voluntary and that the questionnaire was anonymous. No incentives were provided to the group facilitators or participants to promote the dissemination or completion of the survey. The University of Wollongong Human Research Ethics Committee provided approval to conduct the study.
2.4. Statistical analysis
Reliability alpha coefficients were calculated for each of the scales. Spearman’s correlations were used to examine the relationship between the subscales of the Cognitive Behavioural Therapy Skills Questionnaire and the length of time the participant had been attending SMART Recovery groups, the GCQ Engagement Scale, the Quality of Facilitation Scale and the Homework Frequency item. Both the cognitive restructuring and behavioural activation subscales were normally distributed. Two separate regression analyses were used to predict how frequently the participants use cognitive restructuring and behavioural activation, as measured by the Cognitive–Behavioural Therapy Skills Questionnaire. Stepped regression analyses were used to firstly examine the contribution of group delivery variables (i.e. quality of facilitation and group cohesion), followed by the contribution of homework activities. At the first step, the GCQ engagement subscale and quality of facilitation scale were entered as independent variables. At the second step, the frequency of homework item was entered as an independent variable. In both models, the residuals were normally distributed. The length of time that the person had been attending the SMART Recovery groups was not included, as it was not significantly correlated with either the cognitive restructuring or behavioural activation subscales.
3. Results
3.1. SMART Recovery participants
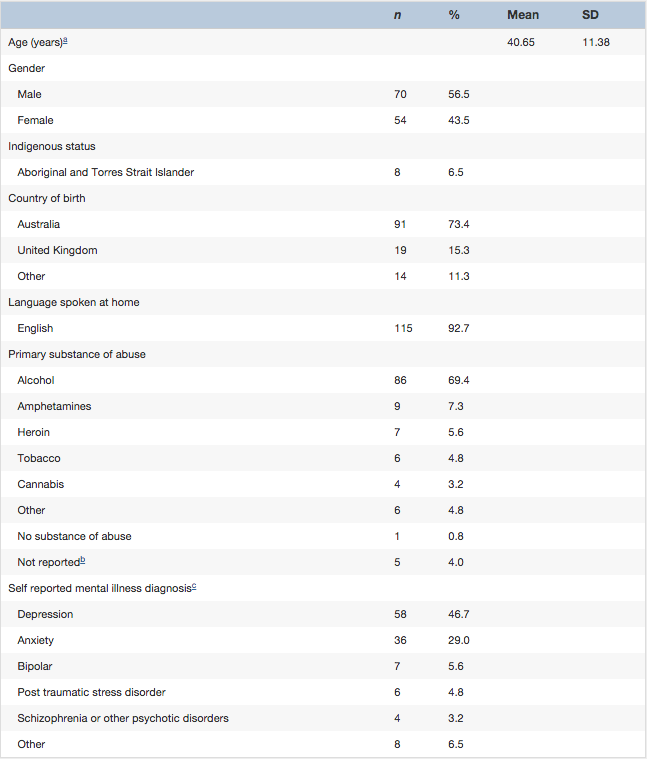
The average age of participants was 40.65 years. More males (n = 70) than females (n = 54) completed the survey. The principal source of income for the large majority of participants was a temporary benefit (n = 28, 22.6%) or pension (n = 38, 30.6%). Twenty-six participants had full-time employment (21%) and 12 participants were employed part-time (9.7%). On average, participants had been attending SMART Recovery groups for 8.78 months (SD = 14.11; range, 1 week to 96 months). The large majority of participants attended groups on a weekly basis (n = 90, 72.8%). One participant (0.8%) attended groups more than 3-times per week, 10 participants (8.2%) attended twice a week, 13 participants (10.7%) attended groups 2 to 3 times per month, and the remaining participants attended monthly or less. In addition to the SMART Recovery groups, participants concurrently attended a range of other treatment options. These included individual counselling (40%), 12-step meetings (17%) and pharmacotherapy services (11%).
3.2. Problematic behaviours
Participants were asked to indicate the problem behaviour(s) that caused them “concern”. Alcohol (72.6%), tobacco (46.0%) and drug addiction (42.7%) were the most highly endorsed items by participants. Other problematic behaviours identified by participants included food (10.5%), gambling (9.7%), shopping (6.5%), pornography (4.8%) and sex addiction (3.2%).
The large majority of participants reported an extended history of problematic alcohol or other substance use problems (99.1%). On average, participants reported having had alcohol or other substance use problems for 18.11 years (SD = 10.97). As highlighted in 1, alcohol was the substance of abuse most commonly reported as providing the “greatest concern” for participants. However, participants reported using a range of substances in the previous 12-months. These included alcohol (85.6% of participants), tobacco (63.0%), cannabis (44.0%), heroin and other opioids (32.3%), amphetamines (27.4%), analgesics (22.6%), cocaine (12.1%), ecstasy (11.3%), and other substances of abuse (3.2%).
3.3. Mental health
Eighty-one participants (66.4%) reported that they had previously attended treatment for a mental health problem. Depressive (41.1%) and anxiety disorders (33.1%) were the most commonly reported diagnoses (see Table 1). Fifty-eight participants (46.8%) reported that they were currently prescribed medication to address a mental health concern. Thirty-six participants (29.0%) reported that they had previously attempted suicide, with only one participant reporting that they had made an attempt in the previous 30-days. The mean K-10 score was 21.74 (SD = 4.91), indicative of a moderate to high score (Australian Bureau of Statistics, 2012). Over a quarter (28%) of participants were classified in the high range (scores between 22 and 29) and 20% were classified in the very high range (i.e. scores 30 and above).
Table 1
Demographic information for participants attending SMART Recovery groups.
3.4. Use of cognitive behavioural skills, group cohesion, quality of group facilitation and homework
On average, participants reported that they would “sometimes” to “frequently” use cognitive restructuring (M = 3.27, SD = 0.73) or behavioural activation (M = 3.11, SD = 0.79). Participants were significantly more likely to use cognitive restructuring than behavioural activation [t(120) = −2.87, p = .005]. Table 2 presents the total mean scores and standard deviations for each of the potential predictor variables and presents the correlations between the potential predictor variables. As the length of time participants had been attending SMART Recovery was not related to either the cognitive restructuring or behavioural activation subscales, it was not included in the subsequent regression analyses.
Table 2
Spearman’s correlations for the potential predictor variables (n = 121).
3.5. Predicting the use of cognitive behavioural skills
Table 3 presents the result of the stepped multiple regression analyses between the cognitive restructuring subscale and the predictor variables. The first step was significant, with the predictor variables as a group accounting for 15% of the variance in cognitive restructuring scores, F(2,113) = 10.90, p < .000. Group cohesion was the only significant predictor (β = 0.31). The second step did not produce a statistically significant improvement in the model (p = .08), with the predictor variables as a group accounting for 17% of the variance, F(3,113) = 8.42, p < .000. Group cohesion remained the only significant predictor in the final model (β = 0.23).
Table 3
Summary of linear regression analysis for variables predicting the use of Cognitive Restructuring and Behavioural Activation. a
Table 3 also presents the result of the stepped multiple regression analyses between the behavioural activation subscale and the predictor variables. The first step was significant, with the predictor variables as a group accounting for 12% of the variance in behavioural activation scores, F(2,113) =8.39, p < .000. Group cohesion was the only significant predictor (β = 0.26). The second step produced a statistically significant improvement in the model (p < .000), with the predictor variables as a group accounting for 21% of the variance, F(3,113) =10.99, p < .000. The homework item was the only significant predictor in the final model (β = 0.36).
4. Discussion
This is the first study to examine SMART Recovery participation within an Australian context. Participants attending these groups presented with a complex clinical profile. On average, participants reported a long history of alcohol or substance abuse (M = 18 years), presented with high rates of co-occurring mental illness (with 29% having previously made suicide attempts), and high rates of unemployment (69%). Encouragingly, on average, participants reported that they ‘sometimes’ to ‘frequently’ used cognitive restructuring and behavioral activation to help support their recovery. The length of time that participants had been attending SMART Recovery groups was not related to the use of either cognitive or behavioral skills. The overall model predicting the use of cognitive restructuring accounted for 17% of variance. Group cohesion was the only statistically significant predictor, with the introduction of homework failing to statistically improve the model. The model predicting the use of behavioral activation accounted for 21% of the variance. Stepping in the homework variable significantly improved the predictive utility of the model.
The current study was correlational in nature, and as such, causation cannot be drawn from the results. However, the results from both predictive models were consistent with the broader psychotherapy literature that has identified group cohesion as being an important aspect of psychotherapy (e.g. Schnur & Montgomery, 2010). It may be useful for future research to examine what contributes to high levels of group cohesion within SMART Recovery groups, as this may help to improve the development and translation of skills. Although participants’ perception of the quality of facilitation did not significantly predict cognitive or behavioral skill utilisation, it was positively correlated with group cohesion (r = .38). It is likely that in addition to the characteristics of group participants (e.g. cooperativeness), the group facilitator will contribute to perceptions of group cohesion, and play a role in helping to develop and maintain group cohesion. Further research needs to be conducted to clarify the role of the group facilitator in promoting group cohesion.
Participants who indicated that they left the group meetings with an achievable plan to be completed between groups were more likely to report the use of behavioral activation. However, the homework ratings did not significantly improve the prediction of cognitive restructuring. It is possible that the types of homework activities developed within SMART Recovery groups are more behaviorally focused. For example, with goal setting being a core component of the SMART Recovery approach, it is likely that homework tends to be more practical and concrete in nature. Future research would benefit from examining the range of action plans commonly developed within SMART Recovery groups (e.g. Kelly and Deane, 2009a, Kelly et al., 2007). Homework administration procedures as part of SMART Recovery groups are currently conducted quite informally. Participants do not routinely leave appointments with their action plans written down, and the plans are not routinely reviewed at the following group meeting. These are both processes that are thought to be part of systematic homework administration which in turn lead to greater homework effectiveness and improved outcomes (Kelly & Deane, 2009b). The quality of homework administration has been found to be related to improved client outcomes (Kelly & Deane, 2009b). It is likely that the effectiveness of the action plans would be enhanced if SMART Recovery incorporated more systematic approaches to developing homework.
There are a number of limitations associated with the current research design that should be considered when interpreting the results. The study was only focused on participants attending Australian SMART Recovery groups, there was a relatively small sample size, and there was a low survey response rate. Additionally, recruitment and procedures for completing and returning the surveys may have produced an unknown bias. For example, it is possible that higher functioning participants returned more of the surveys. Whilst a standard script was provided to the facilitators to introduce the survey, we were not able to monitor the way that the facilitators distributed the surveys. It is possible that the way the survey was introduced to participants may have influenced the way that the participants responded. Additionally, it is possible that some participants may have discussed the survey whilst completing it, potentially influencing their individual responses. All of these variables potentially reduce the generalisability of the results. The study was conducted as a cross sectional survey and was largely correlational in nature. It is therefore not possible to examine causation. All information collected as part of the study was self-report. Future research may benefit from using more objective measures of cognitive and behavioral skill acquisition (e.g. observer rated), as well as examining the quality with which these skills are implemented (e.g. Kiluk, Nich, Babuscio, & Carroll, 2010). The homework measure used in the current study comprised a single item and there is a need for more comprehensive measures that assess both the amount and quality of homework activities. It was outside the scope of the current study to examine the relationship between substance use and the use of the cognitive behavioral skills. However, it would be particularly useful for future longitudinal research to examine the degree to which cognitive and behavioral skill utilisation is related to client outcomes (e.g. reductions in alcohol or substance use and in criminal activity).
SMART Recovery has provided an alternative to 12-step based mutual support groups. The proliferation of SMART Recovery groups across Australia, and throughout the world, highlights the unique role that these types of groups can play as part of alcohol and other substance abuse treatment. Whilst SMART Recovery was initially developed to reflect current evidence based practices in the field (i.e. motivational interviewing, CBT), only very limited research has specifically examined SMART Recovery. It is important that a research base be established for SMART Recovery. The current study provides the first description of what are thought to be ‘active ingredients’ associated with SMART groups. It demonstrates that participants do use a combination of cognitive and behavioral skills, although there is variability across individual participants. Results from the current study suggest that it may be beneficial to consider strategies to improve group cohesion and to better integrate the way that homework is used to support SMART Recovery groups. However, it is important to note that the current study was largely correlational in nature. There is a strong need for longitudinal research to be conducted that examines SMART Recovery participation, and potential outcomes associated with attendance at SMART Recovery groups. As participants attending SMART Recovery report high rates of co-occurring mental illness, it might be particularly relevant to examine the extent to which SMART Recovery also helps to improve mental health symptoms.
Acknowledgments
This study was partially funded by the Community Mental Health Drug and Alcohol Research Network and SMART Recovery Australia. SMART Recovery Australia was advised in the development of the survey and helped to facilitate the collection of the survey data. The interpretation of the data, analysis, writing of the report and submission of the article for publication were all the responsibility of the three named authors.
References
Allwood and White, 2013 Allwood, S. and White, W. SMART Recovery® history. (Retrieved from)http://www.williamwhitepapers.com/pr/2012AChronologyofSMARTRecovery.pdf; 2013.
Andrews and Slade, 2001 Andrews, G. and Slade, T. Interpreting scores on the Kessler Psychological Distress Scale (K10). Australian and New Zealand Journal of Public Health. 2001; 25: 494–497
Atkins et al., 2007 Atkins, R.G. Jr. and Hawdon, J.E. Religiosity and participation in mutual-aid support groups for addiction. Journal of Substance Abuse Treatment. 2007; 33: 321–331
Australian Bureau of Statistics, 2012Australian Bureau of Statistics. Information paper: Use of the Kessler Psychological Distress Scale in ABS Health Surveys, Australia, 2007–08 (4817.0.55.001). ; 2012 (Retrieved 29th January 2014)
Brooks and Penn, 2003 Brooks, A.J. and Penn, P.E. Comparing treatments for dual diagnosis: Twelve-step and self-management and recovery training. The American Journal of Drug and Alcohol Abuse. 2003; 29: 359–383
Dawson et al., 2006 Dawson, D.A., Grant, B.F., Stinson, F.S., and Chou, P.S. Estimating the effect of help‐seeking on achieving recovery from alcohol dependence. Addiction. 2006; 101: 824–834
Deane et al., 2012 Deane, F.P., Mercer, J., Talyarkhan, A., Lambert, G., and Pickard, J. Group cohesion and homework adherence in multi-family group therapy for schizophrenia. Australian and New Zealand Journal of Family Therapy. 2012; 33: 128–141
Gossop et al., 2003 Gossop, M., Harris, J., Best, D., Man, L.-H., Manning, V., Marshall, J. et al. Is attendance at Alcoholics Anonymous meetings after inpatient treatment related to improved outcomes? A 6-month follow-up study. Alcohol and Alcoholism. 2003; 38: 421–426
Horvath, 2000 Horvath, A.T. Smart Recovery®: Addiction recovery support from a cognitive–behavioral perspective. Journal of Rational-Emotive and Cognitive-Behavior Therapy. 2000; 18: 181–191
Horvath and Yeterian, 2012 Horvath, A.T. and Yeterian, J. SMART Recovery: Self-empowering, science-based addiction recovery support. Journal of Groups in Addiction and Recovery. 2012; 7: 102–117
Jacob et al., 2011 Jacob, K.L., Christopher, M.S., and Neuhaus, E.C. Development and validation of the Cognitive–Behavioral Therapy Skills Questionnaire. Behavior Modification. 2011; 35: 595–618
Johnson et al., 2006 Johnson, J.E., Pulsipher, D., Ferrin, S.L., Burlingame, G.M., Davies, D.R., and Gleave, R. Measuring group processes: A comparison of the GCQ and CCI. Group Dynamics: Theory, Research, and Practice. 2006; 10: 136–145
Kazantzis et al., 2000 Kazantzis, N., Deane, F., and Ronan, K.R. Homework assignments in cognitive behavioral therapy: A meta-analysis. Clinical Psychology: Science and Practice. 2000; 7: 189–202
Kazantzis et al., 2010 Kazantzis, N., Whittington, C., and Dattilio, F. Meta-analysis of homework effects in cognitive and behavioral therapy: A replication and extension. Clinical Psychology: Science and Practice. 2010; 17: 144–156
Kelly and Deane, 2009a Kelly, P.J. and Deane, F.P. Do therapeutic homework assignments address areas of need for individuals with severe mental illness?. Community Mental Health Journal. 2009; 47: 194–200
Kelly and Deane, 2009b Kelly, P.J. and Deane, F.P. The relationship between therapeutic homework and clinical outcomes for individuals with severe mental illness. Australian and New Zealand Journal of Psychiatry. 2009; 43: 968–975
Kelly et al., 2007 Kelly, P.J., Deane, F.P., King, R., Kazantzis, N., and Crowe, T.P. A taxonomy for homework used by mental health case managers when working with individuals diagnosed with severe mental illness. Community Mental Health Journal. 2007; 43: 565–581
Kelly et al., 2009 Kelly, J.F., Magill, M., and Stout, R.L. How do people recover from alcohol dependence? A systematic review of the research on mechanisms of behavior change in Alcoholics Anonymous. Addiction Research and Theory. 2009; 17: 236–259
Kelly and Moos, 2003 Kelly, J.F. and Moos, R. Dropout from 12-step self-help groups: Prevalence, predictors, and counteracting treatment influences. Journal of Substance Abuse Treatment. 2003; 24: 241–250
Kessler et al., 2003 Kessler, R.C., Barker, P.R., Colpe, L.J., Epstein, J.F., Gfroerer, J.C., Hiripi, E. et al. Screening for serious mental illness in the general population. Archives of General Psychiatry. 2003; 60: 184–189
Kessler et al., 1997 Kessler, R.C., Mickelson, R.D., and Zhao, S. Patterns and correlates of self-help group membership in the United States. Journal of Social Policy. 1997; 27: 27–46
Kiluk et al., 2010 Kiluk, B.D., Nich, C., Babuscio, T., and Carroll, K.M. Quality versus quantity: Acquisition of coping skills following computerized cognitive–behavioral therapy for substance use disorders. Addiction. 2010; 105: 2120–2127
Li et al., 2000Li, E.C., Feifer, C., and Strohm, M. A pilot study: Locus of control and spiritual beliefs in alcoholics anonymous and smart recovery members. Addictive Behaviors. 2000; 25: 633–640
MacKenzie, 1983 MacKenzie, K.R. The clinical application of group measure. in: R.R. Dies, K.R. MacKenzie (Eds.) Advances in group psychotherapy: Integrating research and practice. International Universities Press, New York; 1983
Magill and Ray, 2009 Magill, M. and Ray, L.A. Cognitive–behavioral treatment with adult alcohol and illicit drug users: A meta-analysis of randomized controlled trials. Journal of Studies on Alcohol and Drugs. 2009; 70: 516–527
Miller et al., 2006Miller, W.R., Sorensen, J.L., Selzer, J.A., and Brigham, G.S. Disseminating evidence-based practices in substance abuse treatment: A review with suggestions. Journal of Substance Abuse Treatment. 2006; 31: 25–39
Moos, 2008 Moos, R.H. Active ingredients of substance use-focused self-help groups. Addiction. 2008; 103: 387–396
Morgenstern and Longabaugh, 2000 Morgenstern, J. and Longabaugh, R. Cognitive–behavioral treatment for alcohol dependence: A review of evidence for its hypothesized mechanisms of action. Addiction. 2000; 95: 1475–1490
Schnur and Montgomery, 2010 Schnur, J.B. and Montgomery, G.H. A systematic review of therapeutic alliance, group cohesion, empathy, and goal consensus/collaboration in psychotherapeutic interventions in cancer: Uncommon factors?. Clinical Psychology Review. 2010; 30: 238–247
SMART Recovery, 2014 SMART Recovery. 2013 Participant Survey Results. (Retrieved from)http://www.smartrecovery.org; 2014.
